Ok folks – starting to get some interest in giveaway items, after a puzzling lull. I’m going to chalk it up to everyone being focused on the events of 6 January. So here are some more items I’m giving away.
The zebra compression socks, camomile tea, and Ugg boots have all found new homes.
This third giveaway will be two foam rollers, given away separately (i.e, two winners).
White foam roller, round, 4″ x 36″
The first foam roller is soft and gently used. It is a CanDo white polyethylene closed cell foam roller, round, 4″ x 36″. 2.0 lb density. This was my first foam roller – I found it to be a bit too soft, as it will deform with use. I’d recommend it to someone who is lightweight and/or wants to try one out, knowing if they like it they might need to buy a slightly sturdier one. It has been used in a fragrance-free, smoke-free home (*not* pet-free – one dog).
Black foam roller, round, 6″ x 36″
The second foam roller is hard and brand-new. It is a CanDo high-density black EPP molded foam roller, closed-cell, round, extra-firm, 6″ x 36″. This molded foam is firmer and more rugged than polyethylene foam. Goldilocks time: this roller was too hard for me. I would not recommend it for folks with fibromyalgia, based on my experience. I found this roller very painful. But it obviously works for some folks. It is a very firm roller, and should withstand higher weight individuals without deforming. This foam roller has been in a fragrance-free, smoke-free home (*not* pet-free – one dog).
If you are interested in either foam roller, please leave a comment letting me know which one you’d like to win. I will leave the contest open for ~ 1 week, since we chronically ill/disabled folks operate at a slower pace (in most cases). Sorry -U.S. residents only, since I’m paying for the postage.
The events of 6 January 2021 were deeply disturbing. I was going to space these giveaways out a bit further, but I think we could use some comfort. So I’m giving away several more items that will hopefully bring a bit of comfort. If you are interested in any of these items, please leave a comment and specify which one of the items you’d like. To be clear, I am giving away three (3) items, separately.
Second Giveaway:
A gently used cream-colored fuzzy robe [synthetic material] with pockets. 48″ long. Probably men’s medium/women’s large. Scratchy tag removed, but the robe can be safely machine washed and dried. Previously washed with fragrance-free detergent (Seventh Generation Free & Clear); possibly previously dried with Bounce Free & Gentle dryer sheets or fragrance-free wool dryer balls.
Sealed tin of organic Chamomile tea, with images of chamomile flowers on a yellow background
3. A pair of new, never-worn Ultra Short Ugg boots women’s size 9/men’s size 7.5. Chestnut color. Suede leather outside. Shearling inside. [Made from actual wool – avoid if you are allergic/sensitive to wool] Removable, replaceable insoles. Waterproof soles.
A pair of Ugg boats, with sole showing the brand mark
All items come from a fragrance-free, smoke-free home. Home is NOT pet-free– there is a dog.Bonus: Packages may include random black dog hairs.
Again, please leave a comment if interested, and specify which item you’re interested in. I plan to give y’all a week to enter before I select the winners. I would strongly prefer that these items go to chronically ill and disabled individuals who can use them. I am not gatekeeping illness/disability, but if you are abled, please don’t be a dick and take these items from chronically ill/disabled people who could use them – this giveaway is not for you.
So, I have picked a word of intention for 2021, and it is Curate. Rather than being stuck in frustration, disappointment, and anger that my plans for the next phase of my life have been derailed by my chronic illness/disability, I am trying to reframe it as an opportunity to curate my life by letting go of things that no longer serve me, whether that is former ambitions, emotional baggage, or physical possessions.
When I was busy chasing after goals, I didn’t spend much time being introspective, nor did I spend time dealing with the stuff I’d accumulated. But now I have time…so I’m working on rightsizing my life and making sure it aligns with my values.
Toward that end, I have decided to give away things that I do not need, but which other people might need and/or enjoy. All of these items are either new or gently used.
I’ve never done an online giveaway before, so I’ll be learning as I go. Please bear with me.
Here’s the first giveaway: A pair of L/XL ProCompression zebra-striped compression socks. According to ProCompression, these socks will fit men’s size 11-13, women’s size 11-14, and a 16-20″ calf-size. These socks are new, in the packaging.
So, if you could use a pair of compression socks, leave a comment. I’ll select one winner. [Sorry, U.S. residents only, since I’m paying for the postage.]
One way I am learning to manage my health since becoming chronically ill/disabled is to break things down into smaller chunks or easier steps. Rather than becoming overwhelmed by tasks that I no longer have the mental, physical, or emotional energy to complete, I am very slowly learning to accept that I must alter my expectations and adapt my mindset and my behaviors.
So last month when I was talking to My Boomer Parent and they mentioned reading that a ten-minute walk was sufficient to help control/reduce blood sugar [glucose], I was intrigued, if skeptical.
Spousal Unit & I do not have diabetes, but many of our relatives do, so I decided to dig into the research. What I found was that My Boomer Parent was right: a 10 minute walk after eating helps regulate blood sugar. In fact, according to one study conducted by researchers at the University of Otago, New Zealand:
“When the participants walked for 10 minutes after each meal, their blood sugar levels were an average of 12% lower than when they took a single 30-minute walk each day.”
The idea of ten-minute walks was a lightbulb moment for me. I have been struggling to get sufficient exercise that won’t be counterproductive by aggravating my health conditions. For example, I used to love to run when I was young. When I could no longer run, I began walking. I would walk for a minimum of 45 minutes to an hour, at a brisk pace, and found that to be a great stress-releaser.
But now my joints just can’t handle that. Since moving to Florida, I have been walking about a 1 mile loop, and then my knees and SI joint are so sore and inflamed that I have to ice my knees and put a heating pad on my back, and it makes me less able to do things for a couple of days, which is not only counterproductive, but also frustrating and embarrassing.
But ten minutes? I can walk for ten minutes! And if it doesn’t inflame my knees, then I can even do it regularly. In fact, I might be able to work up to doing it several times a day.
Research shows that it’s beneficial to walk for ten minutes after each meal. But it also shows that the most important time to walk might be after dinner.
Taking a short walk after dinner showed the greatest benefit on blood glucose, particularly when the meal contained a lot of carbohydrate, lowering blood sugar levels by 22% compared to taking a single daily walk.
So I started out with a ten minute walk after dinner. And my knees didn’t hurt. (My SI joint was already out of position, so I considered it a wash that it was a little sore afterward.)
My initial plan was to walk after dinner every night for two weeks, and then to evaluate whether I could add a walk after breakfast. Lunch might be difficult, as we’re headed into Summer here in the Northern Hemisphere and I don’t do well with heat. But we’ll see how it goes. Perhaps I can handle ten minutes’ worth of heat.
Update: I’ve been walking for a month now. It has become a streak, and is well on its way to becoming a habit pattern. Ten minute walks after dinner are working really well for me. I set an alarm for 30 minutes after dinner, because the Otago study stated that “undertaking activity after waiting for 30 min following eating might be optimal in modifying the glycemic response.”
I find that ten minute walks are both physically *and* psychologically easier than longer walks. I don’t have to change into exercise clothes. I don’t have to carve out a large block of time. I seldom have to apply ice or heat afterward. Even on days when I’m very fatigued or my symptoms are flaring, I can manage a 10 minute walk.
Previously, I often had days when I did not feel well enough to do a 1 mile walk. And what do you do when you get halfway through a walk and don’t feel well enough to get home? But now I have a route that extends a little way past my home in both directions, so I am never very far from home. If I *really* wasn’t feeling well, I could just turn around and get home quickly.
It may sound ridiculous to able-bodied people. It might sound ludicrous to the veterans with whom I served, most of whom are still running marathons and doing triathlons. But 10 minute walks are what I am capable of, and they are what works for me.
Rather than feel bad that I can no longer run 10Ks, I choose to feel good that I have found an exercise that is working for me and has scientific evidence of efficacy. Instead of focusing on all the things I can no longer do, I choose to focus on the things that I can still do to manage my health.
Crew Dog, onesickvet.com
After one month, I have not added a second daily walk yet. Instead, I am working on adding home physical therapy to my daily routine. Right now, I am very inconsistently trying to do 10 minutes of exercise ball core strengthening exercises per day. I think I need to establish a set time to do these exercises in order for it to become a successful habit, in the same way that the walks are consistently 30 minutes after dinner every night. I don’t forget to do the walks, because there is a set time for them every day.
I also find the “streak” aspect very motivational. Some days I really don’t feel like going for a walk, but I don’t want to break the streak. So I go.
In summary, I am finding the idea of “only” doing something for ten minute at a time to be very powerful and productive. We have 1,440 minutes in a day. Surely I can take ten of those to do something healthy for myself? And then I can take another ten minutes somewhere else in the day to do something else healthy for myself, and gradually I can build healthy habits that are small and easy enough that I can consistently accomplish them.
And so I am using the power of ten minute time chunks to manage my limited energy. I don’t have to run a marathon – I just have to walk for ten minutes after dinner. I don’t have to climb El Capitan – I just have to do ten minutes of core strengthening after I wake up each morning.
And so it goes. I am taking positive actions for my physical and mental health, ten minutes at a time. And I think this could work for almost anyone. Able-bodied but working a frantic schedule? Carve out ten minutes for your health. Stay at Home parent? Find ten minutes for your health.
You know what? Some people are more disabled than I am. Maybe ten minute chunks won’t work for them. That’s ok – break it into smaller chunks. One minute of isometric exercises in your bed. Whatever works for you.
I am sensitive to peoples’ varying needs and abilities – if you can’t do anything, then don’t. The objective is to take care of oneself. I’m just sharing a technique that was a breakthrough for me.
BOTTOMLINE:Using ten minute micro walks, I have gone from walking once or twice a month to walking every night. My average mileage has increased, and I’m getting consistent daily exercise. I am literally and figuratively learning to pace myself. I am now using the ten minute technique to add additional healthy habits to my life.
I won’t be blogging much about COVID19 here, but I am re-tweeting excellent content from doctors, epidemiologists, scientists, health organizations, and even personal finance bloggers on Twitter, so if you want COVID19 content from informed sources you can follow me @onesickvet . Or see the Twitter feed on this blog.
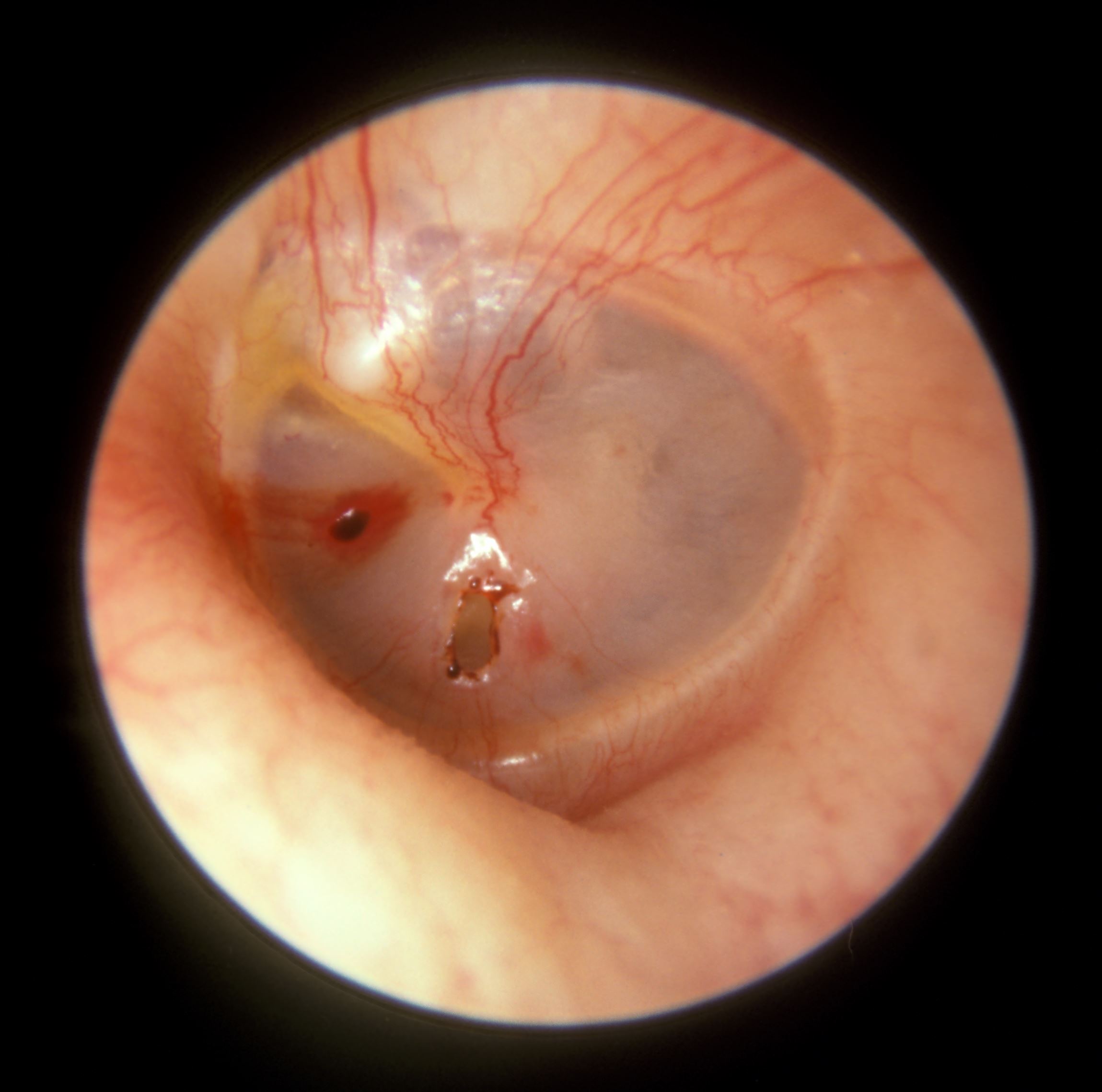
(Not my actual ear. My injury looks like the hole, not the tear.)
I would prefer not to know this from firsthand experience, but here I am.
I have been scuba diving for over 25 years, almost completely without incident until this week. [Yes, the slip & fall incident happened on a Scuba vacation, but it happened topside, not in the water.]
It started like any other dive: Spousal Unit & I were diving with a new group of people, and we waited for everyone to get in the water and then we all descended. I had no problems clearing my ears on the descent. We had a mellow dive, checking out a new reef. When one of the divers in our group reached 1,000 psi of air remaining, we started our ascent. I was in no particular hurry to ascend, as I still had plenty of air in my tank.
But at 20 feet below the surface, my ear started hurting. I leveled off (stopped my ascent), and worked my jaw. Next, I massaged the area under my ear where my eustachian tube is, but my ear still wouldn’t clear. Not realizing that my problem was too much pressure in my ear, rather than not enough pressure in my ear, I did a valsalva maneuver. My ear still didn’t clear. More jaw rocking, more eustachian tube massaging – still nothing. So I did another valsalva maneuver – and my eardrum perforated.
I felt and heard a loud pop in my affected ear, followed by a sensation of cold water rushing into my ear. The pressure equalized, and my ear pain lessened significantly. But I suspected that something very bad had just happened.
Crew Dog, www.onesickvet.com
I did not see any blood or mucus in the water, but usually when my body pops, it means something ruptured. Since my ear had equalized, I resumed my ascent up to the 15 foot safety stop and caught up with the rest of my group.
During the safety stop, I continued to troubleshoot my ear. I did another valsalva maneuver, and heard and felt air escaping through my ear – I could hear and feel the air transiting my eardrum, and then I could hear and see bubbles coming from my ear. That pretty much confirmed to me that I had perforated my eardrum.
During the safety stop at 15 feet below the surface, I had a huge wave of vertigo wash over me, and I became very disoriented. Disorientation can be very dangerous when you’re diving; however, I was in a group, at 15 feet, and I could see the surface. And I have a lot of experience with vertigo, since I’ve had Migraine-associated vertigo for ~ twenty years. I decided to maintain the safety stop, rather than immediately ascend to the surface, so that I did not create any more physiological problems.
[I am not advising anyone else on what they should do in this situation, I am merely relating my own thought process.]
Thankfully, the vertigo slowly subsided, and I was able to safely ascend. At the surface, I told Spousal Unit that I thought I had ruptured my eardrum. Spousal Unit looked at my affected ear, but did not see anything unusual.
We returned to the boat and took off our gear. Spousal Unit still didn’t see anything unusual, although I did another valsalva maneuver and Spousal Unit could hear air escaping my ear with a whistling noise. The group started getting ready for the second dive. I started to question whether I had really ruptured my eardrum – it really hadn’t been that violent. In fact, it had been somewhat subtle. I briefly contemplated getting back in the water – we were supposed to be doing two dives for a specialty certification, and I wanted to finish the training.
Here’s what the mental math looked like:
Pros:
Log the second dive and perform the necessary skills to complete my specialty certification.
Cons:
Might not be able to clear ears on descent or ascent.
Might get disoriented at depth, leading to a possibly life-threatening situation.
Might get an inner ear infection if eardrum *is* ruptured and bacteria get behind the eardrum/inside the ear.
I decided discretion was the better part of valor, and I should sit out the second dive.
Next, I informed the instructor that I believed I had ruptured my eardrum. I was not prepared for his response – he did not seem to believe me. He asked if there was any blood or mucus. He looked at my ear. He said, “Sometimes my ear crackles; are you sure it wasn’t just that?” He did not pressure me to get back in the water, but it was clear he didn’t believe I had actually ruptured my eardrum. He said something to the effect of, “Most people, when they rupture an eardrum, are screaming in pain and vomiting.”
Even though I knew sitting out the second dive was the more conservative course of action, it was still difficult to stay onboard the boat. I had never sat out a planned dive before. I felt guilty and like a slacker because I left Spousal Unit without a buddy, and because no one seemed to believe my injury.
[For the record, Spousal Unit was completely not bothered to be diving without me, and agreed that staying out of the water was the right choice.]
So I sat on the boat while the rest of the group completed their training on the second dive. And even though the seas had calmed considerably after our first dive, I was feeling very nauseated. So, I sat on the boat cold, wet, and queasy, determined that I was NOT going to vomit.
Meanwhile, I had noticed that the tinnitus in my injured ear was orders of magnitude louder than usual, and that my hearing was very muffled in that ear. Again, tinnitus was a pre-existing condition for me, but never had it been this bad. And muffled hearing sometimes was a part of my tinnitus symptoms, but never this extreme.
After the group completed their second dive, we returned to the dive shop. On the boat ride back in, I spoke to the instructor about getting medical care. Since it was the Sunday of a three-day weekend, and we don’t know any ENTs in the area, not having lived here that long, I was hoping he’d have some suggestions.
The dive instructor coordinated for me to talk on the phone with a retired military flight surgeon (they know a lot about ears and pressurization problems), and after our consult, she confirmed that I had probably perforated my eardrum, meaning there was likely a hole, but not a large tear across the membrane. She recommended I see my GP (general practitioner) the following day, since they would not be open on a Sunday.
However, since it was a holiday weekend, I didn’t think my GP would be open on Monday either. After we got home, I did some internet sleuthing and even called the office, but the recording didn’t say whether they would be open on MLK Day or not.
But, the recording *did* have the number for the 24 hour nurse care line, which I called. The nurse was not experienced with perforated eardrums, but decided that I should go to Urgent Care when they opened Monday morning (since they had already closed for the night), and authorized an Urgent Care visit.
After very carefully inserting an ear plug in my damaged ear, I took a shower and washed all the salt water off, and then I resumed my internet research.
According to the Mayo Clinic and emedicinehealth, my symptoms matched the symptoms for a perforated eardrum*; a perforated eardrum will usually heal itself; and an infection in the inner ear is really bad and could lead to permanent hearing loss (among other things), so you should treat with antibiotics, especially if your ear was underwater when the eardrum ruptured.
*Symptoms of a Ruptured Eardrum:
Feeling something is not right with the ear
Ear pain that may subside quickly
Clear, mucuslike, pus-filled, or bloody drainage from your ear
Hearing changes/hearing loss
Ringing in your ear (tinnitus)
Spinning sensation (vertigo)
Nausea or vomiting that can result from vertigo
Feeling comfortable in my decision not to go to the emergency room, but to go to urgent care in the morning, I took an OTC pain reliever and went to bed. The next morning, after confirming that my GP’s office was closed but Urgent Care was open, off we went to Urgent Care.
I was seen by a PA, who bounded into the room saying, “I wanted to see this!” After I recounted my story to him, he took the otoscope off the wall, looked in my ear, and said, “Yup! There it is!” And he offered Spousal Unit the chance to look, which Spousal Unit took him up on. [I was envious, and wistful that I could not see inside my own ear.]
[Geek moment: The PA first examined my good ear, upon which, I exclaimed, “Cool! I am my own control group!”]
The PA confirmed what I had read online: I cannot dive until the membrane has fully healed; it *is* safe to fly with a perforated eardrum; I should take antibiotics to hopefully stave off any potential infection; and I should keep my ear dry while it is healing, including using an ear plug in the shower.
He told me that I had a pinhole perforation, meaning that it was quite small, and that it would therefore hopefully heal much more quickly and easily than a large rupture. And he wrote a prescription for oral antibiotics and for antibiotic ear drops. He also gave me the phone number for an ENT, and recommended I follow-up with them, although he couldn’t tell me a timeframe for doing so. [I’ll either get authorization from the VA to see an ENT, or I’ll self-refer through Tricare Select, and make sure the ENT gives me a clean bill of health before I dive again.]
Finally, I went to the pharmacy to pick up my prescriptions, and the pharmacist told me that the oral antibiotic that was prescribed has known cross-reactions in people with chlorhexidine allergy (IOW, because I am allergic to chlorhexidine, I might have an allergic reaction to the prescribed antibiotic even though it does not contain chlorhexidine). So the pharmacist diligently determined which antibiotic would be safest for me (ruling out several due to known or possible allergies), and called Urgent Care to change the prescription. The pharmacist also double-checked to make sure the antibiotic ear drops would be safe for me.
I am grateful for the pharmacist’s diligence, as the *last* thing I want is a life-threatening allergic reaction while dealing with a perforated eardrum.
I am currently on day four of five of the antibiotics regimen and have had no problems, for which I am very grateful.
My outer ear and the area below my ear were inflamed (red and swollen) for about the first 18 hours or so; I assume it was white blood cells and mast cells reacting to the injury. The PA also said my inner ear was a bit inflamed when he looked at it. The profound hearing loss/very muffled sensation lasted for about 24 hours. I have regained some of my hearing in that ear since then, although there is still hearing loss and a muffled sensation. I continue to have some balance problems and episodes of dizziness, although they are very mild compared to my usual episodes of vertigo.
After Action Report (AAR):
Leveling out (stopping the ascent) once I realized I was having problems equalizing the pressure in my ear was a good first step, but what I should have done when that wasn’t enough is slowly descend (reverse direction) until I no longer felt pressure/pain in my ear, and then slowly ascend while trying to equalize, re-descending as necessary to avoid putting too much pressure on the eardrum. I now know (and will never forget) that if I (or anyone else) is having a problem equalizing the pressure in one or both ears, the correct course of action is to reverse the direction one was going until the pain/pressure stops. Then keep an eye on your air gauge (to make sure you don’t get too low on air) and work the problem.
Also, always trust your gut. I knew my eardrum was perforated even though there were no outward signs that anyone could confirm. Had I tried to do a second dive, very bad things could have happened.
According to my online research, I will likely be beached for about two months while my eardrum heals, barring any complications. I intend to wait until it is full healed and I have clearance from an ENT doctor before I resume diving. I have heard of other divers who started diving again before their eardrum was fully healed, and they wound up doing more damage and being unable to dive again. I would rather have this be a short hiatus from diving instead of the end of my diving days.
Have you ever had a perforated/ruptured eardrum? What was your experience like? How long did it take you to heal? Please comment below:
I read a couple of interesting pieces today. In the first, Megan Klenke shares her honest thoughts about becoming chronically ill. She talks about being a dancer whose body betrayed her such that she cannot dance. As if this fundamental, existential betrayal weren’t enough, chronic illness has taken even more from her:
“Chronic illness has stolen my body, it has stolen my ability to think clearly, it has stolen my choices, it has stolen my relationships, it has stolen my freedom, it has stolen my safety, it has stolen my identity…what else is there to say?”
Megan Klenke, Why Being Honest Is Hard For Me, No End In Sight
In the second piece I read today, Jill Cornfield writes about the lessons learned by Chanel Reynolds and Liz Gendreau about ways to prepare for unexpected events like sudden death or disability. The combined message from these two pieces is that you never know how much time you have, and the unexpected is easier to deal with if you’re prepared.
What I mean by prepared is not the Zen koan-like saying to “Expect the Unexpected” – we all get blindsided by “unknown unknowns.” As Chanel and Liz explain, there are tangible things we can do to prepare for unexpected expenses, health problems, and even death, such as having an emergency fund, a will, an advanced medical directive (such as a living will), and a croak binder (we first encountered the term in a USAA Magazine article. Apparently it’s a commercially-available product, although you could also DIY it – for ideas, see this article).
After making a list of ways that I need to update my preparedness:
update will/living will
create a Croak Binder
look into bundling insurance policies
I started thinking about another way that chronic illness/disability/death affects us – when someday becomes never. When you or a loved one become chronically ill/disabled, or a loved one dies, certain dreams that you hoped and planned to accomplish someday become things you will never do.
And I don’t want to debate with people who will argue that this is pessimistic and defeatist, and that “you can do anything if you put your mind to it” or “the only disability is your attitude.” No. We, in the wealthiest nations in the world, want to believe that anything is possible, and are often uncomfortable with the frank acknowledgment of limitations, but the harsh truth is that limitations exist. Acknowledging this doesn’t make me a pessimist; it makes me a realist. Disability does not mean we aren’t trying hard enough or don’t want it badly enough; disability literally means nothaving the capacity.
Some of us lose or never had the capacity to enact certain dreams. Megan had the dream of being a professional dancer, but she lost the capacity to do so. And having the dream without the capacity was too painful, so she eventually had to surrender the dream. [I assume.]
I had the dream of obtaining a PhD and helping the military develop leaders, but I lost the capacity to finish my studies and complete the degree. I have withdrawn from my degree program, but I am still struggling with surrendering the dream.
Even more starkly, when a loved one dies there are clearly dreams that will never be enacted – you will never take that trip together to Paris, or have that loved one at your wedding, etc.
But, I would suggest, once you have come to terms with these losses/limitations and realized that certain somedays have become nevers, you can lighten your load by getting rid of (at least some of) the things that you accumulated for someday.
Those hobby/craft supplies you were saving for someday when you would actually put them to use? If it’s been years and you’ve never used them/never finished the project, or you are no longer physically able to do the hobby/craft – let them go.
Those clothes you’ve had shoved in the back of a drawer or the closet because you’re going to lose the weight someday? If it’s been years, that’s probably not happening – give them away.
In my case, it was readily apparent that I was unable to maintain the large house we were living in, and unable to extend hospitality to others in the way we had planned. And I had to admit that “someday I’ll be healthy again and we can do this” had become increasingly unlikely. And so we sold our large house on acreage and moved to a much, much smaller house on a much, much smaller lot.
“In many ways, chronic illness/disability feels like the aging process was accelerated for me. I have the diminished capacities and the diminished prospects of someone twenty to thirty years older. I have fast-forwarded past my anticipated second career into retirement. Like someone decades older, I have downsized and moved to Florida. “
Crew Dog, One Sick Vet
No longer living for someday applies to our finances as well, in ways you may or may not expect. For example, if I lack the capacity to become a Doctor of Philosophy, do I really need to continue my memberships in various professional organizations? Or can I save money, time, and energy by discontinuing these memberships and no longer paying to attend professional conferences?
If we live in a much smaller house and my health limits interactions, can we get rid of some of the furniture we had for guests? Yes. And so we sold a bedroom set before we moved, and we recently sold a set of bunk beds we’d brought with us (after I finally accepted that we really don’t have room for it and probably don’t need it).
By accepting that someday means never for certain things, I am becoming able to get rid of things that are cluttering my house and my mind, and I am gaining freedom by shedding financial, emotional, and physical burdens.
Accepting one’s limitations means that, for some things, someday becomes never, but for other things someday becomes now. Do it now before you lose more capacity. And so I am working on scuba certifications that I didn’t make the time for before. I may or may not have the capacity to use these certifications to help others enjoy scuba when I am done, but I am enjoying the process of learning new things, improving my skills, and becoming a better diver. I may need to use a cart to haul my gear to the water, rather than carrying it, and I may need other aids as my capabilities diminish, but I am going to do what I can while I can.
Do it now because you’re not guaranteed tomorrow. And so I am passing family heirlooms on to the next generation now, before I am gone and cannot pass along the history and the heritage that goes along with the item. And I intend to scan the family photos and write down what I know about the people in them, so that that knowledge isn’t lost. After I’ve done that, I’ll offer the original photos to family members who might want them. And then I’ll no longer be responsible for caretaking them, and I won’t need space to store them.
I had not intended to shed possessions, responsibilities, or dreams at this point in my life – I thought I had much longer before I would need to do so. But there is peace and freedom to be found in surrendering to what is, rather than continuing to long for what cannot be.
However, grief is very much a part of this experience, and it is not linear and it does not follow a timeline. Grief is messy, and it may be expressed as anger, depression, pain, denial, regret, or many other feelings or behaviors. I continue to process my grief over the somedays that have become nevers – the dreams that I will never realize, the things that I will never do, the opportunities that I lack the capacity to pursue.
But when I stop fighting and accept what is, when I release my expectations, hopes, fears, and dreams, when I let go of the things I’ve been hauling around for someday or “used to be,” I find freedom. I find moments of peace and sometimes even joy.
So I’m trying to stop living for someday, and instead just live in the now.* For me, the important part is managing my expectations. If I let go of the dreams and ambitions I held, the expectations for how my life was going to be/supposed to be, I can appreciate that what I have is still pretty darn good.
[*Don’t get me wrong, as far as I know my conditions are chronic, not terminal, so I still have to be responsible with my money and plan for the long-term financially.]
Which reminds me: I’m not saying that having ambitions, goals, plans, or dreams is bad. I’m definitely not saying that these things are only for the abled. I guess what I *am* saying is that nearly all of us have things that we plan or hope to do someday. And those things may be inspirational and motivational. But sometimes waiting for someday interferes with the way we are living now, and then we are faced with a choice: do we keep pining for someday, or do we start living for today?
In my case, I find that I am mentally healthier when I acknowledge that certain things I had hoped and planned to do someday are no longer probable, and I adjust my expectations accordingly.
I may not be living the life I dreamed of, but I intend to live the life I have to the best of my abilities.
I’ve been using home oxygen (at night, while I’m sleeping, supplied by the VA) for the past 2.5 years. Today I learned that my oxygen system has been non-compliant with VA safety requirements since September 2018.
UPDATE: Spousal Unit found paperwork indicating that the oxygen personnel at my gaining VA *did* try to contact me after I arrived. Apparently in the confusion of the move and dealing with my poor health, I misunderstood that they were calling about more than the delivery of the equipment, and I failed to return their missed call. I publicly admit that this failed hand-off was likely my fault, not the VA’s.
After much frustration and confusion, today I received my home oxygen equipment in Florida. 13 months after I relocated. Apparently the hand-off between the Colorado and Florida VA hospitals failed, and my gaining hospital was *never notified* that they were gaining an oxygen patient.However, I didn’t know that becauseI was supplied with an oxygen concentrator upon arrival in Florida. I *did* think it odd that the supplier never returned to refresh my hose stock or to service the machine, as the Colorado supplier had, but I had a few extra hoses and cannulas and I had bigger problems to deal with (like my gaining PCM refusing to renew my medication prescriptions and not referring me to the required specialists for continuing care at my gaining VA hospital).
But I finally got most of those problems resolved, and so my attention shifted to the oxygen supplier mystery. Recently, while I was at the VA hospital for an (unrelated) appointment, I started asking questions about the oxygen situation. This rapidly brought me to the attention of the nurse manager of the home oxygen program at my VA hospital, and he freaked the heck out when I explained the situation to him. He explained that he had never been notified that his hospital was gaining me as an oxygen patient (despite my having worked with a VA patient transfer specialist in Colorado for the move). I had been in Florida for a year, and my local VA home oxygen program had no knowledge of my existence.
Upon learning of my existence, this nurse manager (himself also a veteran) sprang into action. He called me that day, as I was on my way home, and gave me his personal cell phone number. He established exactly what I needed, and made arrangements for the acquisition of necessary equipment even though he was out-of-town (not in the office). In less than a day-and-a-half, he had arranged for delivery of everything I needed. His care has been exceptional, and I cannot say enough good things about him.
So today the oxygen supply company delivered my equipment. Again, excellent service. And as the technician was setting up my equipment and explaining everything, I noticed that the equipment looked a bit different from what I was used to, and the technician was saying that he was installing the fire-safe valves. Which led to a discussion about what they were and how they worked…
And, according to this firesafe cannula valve introductory video, the VA has required their use since 2018:
Fire-safe valve
This was news to me, since I had never seen or heard of these valves until today, despite having been provided oxygen equipment and equipment servicing through the VA throughout 2018 (the year the policy took effect) and 2019. So I did some further research and found VA Patient Safety Alert AL18-01, dated March 12, 2018, which states that “use of thermal fuses may reduce the severity of fires involving home oxygen delivery systems,” and lays out a timeline for the notification of providers and the modification of existing contracts to reflect that the use of thermal fuses IS MANDATORY for all VA patients (AL18-01, pp. 3-4). Furthermore, the Safety Alert requires that “by COB September 21, 2018, the Patient Safety Manager must document on the VHA Alerts and Recalls Web site (http://vaww.recalls.ncps.med.va.gov/WebRecalls/Recalls.html) that medical center leadership has reviewed and implemented these actions [italics added by me].”
Now, I was always very satisfied with the service I received from my VA-contracted oxygen equipment supplier in Colorado, but they certainly were not in compliance with this directive by this deadline, since I left Colorado in October of 2018 and had not been equipped with this new safety item nor informed of the fact that a device existed that would make my home oxygen use safer.
According to this directive, there should be two fire-safe valves in each oxygen delivery system – one near the machine, and one near the user (see diagram, AL18-01, p. 7).
As you can see, my old set-up did not have a fire-safe valve near the machine *or* near my head – the hose (with no thermal fuse) ran from the machine…
…and attached to the cannula with a regular connector (not a fire-safe valve).
Whereas my new machine has a pigtail cord attached to the machine with a fire-safe connector to attach to the hose…
…and the hose attaches to the cannula with a fire-safe valve connector:
So my new system is in compliance with the VA Patient Safety Alert.
Since I consider myself fairly well-informed about my healthcare matters, it was a bit shocking to discover today that this safety device existed and was required by the VA, but I’d never heard of it. So I’m passing this information along to you.
IN ORDER TO REDUCE/PREVENT SERIOUS BURNS FROM FIRES FED BY HOME OXYGEN, MAKE SURE YOUR OXYGEN DELIVERY SYSTEM HAS PROPERLY-INSTALLED FIRE-SAFE VALVES. AND DO NOT SMOKE OR HAVE HEAT SOURCES OR OPEN FLAMES NEAR YOUR OXYGEN EQUIPMENT.
NOTE: You can find more information about home oxygen use here and more information about fire safety & home oxygen use here.
I visited my physical therapist today (which is to say that since we were back in the town where we used to live, I scheduled appointments for myself and Spousal Unit). Although I had been seeing my PT for several years, this was Spousal Unit’s first time receiving treatment from her.
While we were there getting treatment, my PT mentioned that she had a new device that was supposed to help reduce inflammation, and offered to let Spousal Unit and me try it, if we were interested.
So after we had completed our other treatments, we each took a turn trying full body red light therapy, which consisted of going into a private room, taking off all of our clothes except our underpants and our socks (because cold floor), and standing between two red light panels for 10 minutes.
The two panels were parallel to each other and set about two foot apart. One panel was taller than the other. The larger one was about the size of a narrow full-length mirror, and the other panel was the same width, but about a foot shorter. I stood between them for ten minutes, switching to face the other panel halfway through (at the five minute mark).
Due to my chronic migraines and attendant light sensitivity, my PT suggested I wear my dark sunglasses during the light therapy. I began by facing the shorter panel. The light was bright even through my sunglasses that block 97% of light, but it was tolerable.
Initially, I felt discomfort in my digestive system as the light therapy began. It intensified to the point that I wondered if I could endure the full session, but then the discomfort dissipated. I also felt pain in my left elbow, which also intensified and then dissipated. After that, I didn’t have any more pain or discomfort.
I *did* feel warmth to the point that I nearly began to sweat, even though red light therapy is not intended to be particularly heating, as compared to an infra-red sauna, which is intended to be very warm.
After five minutes, I turned around so that I was facing the taller panel. The light on my eyes was more intense, since the top of the panel was directly at eye level, but it was tolerable with my very dark sunglasses on and my eyes closed.
After I completed my full body red light therapy session, I put my clothes back on and went back to the waiting area while Spousal Unit had a turn.
I experienced the following effects after full body red light therapy: I noticed that my lower back was less stiff when I was getting re-dressed than it had been prior to the red light therapy. I felt temporarily nauseated for less than five minutes while I was waiting in the waiting area afterward, but then it passed. I was also very thirsty, but I am typically thirsty after PT, so it’s hard to say whether my thirst was intensified by the red light therapy or not. So most of my symptoms were minor and (very) short term. However, I did feel muscle weakness for about two hours afterward. Spousal Unit reported feeling warm, but no other effects.
My PT did not charge anything additional for us to try this new therapy, although I did notice that her rates had increased by $5 since my previous visit approximately 6 months ago.
After I got back to our camper, I did some research into full body red light therapy, and so far, it is considered experimental and likely safe. Like many other health products, it claims to treat many different ailments. Based on my research, the strongest scientifically-supported claims seem to be for reducing inflammation and stiffness. Since I have chronic inflammation, it is possible that I might find some relief from using red light full body therapy. If you are considering using this therapy, please do your own diligence in investigating the strength of the claims for your particular condition. Given that red light therapy is still experimental, also consider whether the cost is worth it to you – there may be other, proven, therapies that might benefit you more.
If you decide to try it, consider taking a pair of sunglasses, and consider that your hair will need to be up out of the way so that the light can reach as much of your skin as possible. My PT said that many patients read their phones while receiving red light therapy, but I didn’t since I wanted to expose as much of my skin as possible and because my very dark sunglasses are not prescription, so I wouldn’t have been able to read my phone anyway.
My PT had a Joovv brand red light therapy device, but there are other manufacturers of red light therapy devices, both for commercial and at-home applications.
CAUTION: IT IS POSSIBLE TO BURN YOURSELF OR CAUSE DAMAGE TO YOUR EYES with at-home red light therapy devices if you are not careful. *Please follow all manufacturers’ instructions.*
NOTE: Red light therapy is also known as photobiomodulation (PBM), low-level laser therapy (LLLT), cold laser therapy, and many other names.
NOTE: Because red light therapy is considered experimental, it is not FDA approved for most conditions, and it is not covered by healthcare insurance, meaning they will not pay for it.
NOTE: Prior to red light therapy, I had also received manual manipulations, damp heat, and interferential electric nerve stimulation (e-stim) therapy during this visit.
BOTTOMLINE: If you have rheumatoid arthritis or other joint pain or inflammatory conditions, red light therapy may provide modest short-term relief of pain and inflammation. Red light therapy currently appears to be considered likely safe when used correctly.
The information contained in this article is for educational and informational purposes only and is not intended as health or medical advice. Always consult a physician or other qualified health provider regarding any questions you may have about a medical condition or health objectives.
I haven’t posted much lately, so here’s a quick update. I’ve been trialing Xolair, a medication that my allergist hoped would improve my quality of life. It did not have the specific effects that my allergist had hoped for, so she recommended I discontinue it. [*For my experience with Xolair, see the end of this post]
At the same time, and against my better judgement, my allergist wanted me to discontinue another medication. I try very hard to only change one variable at a time, so that I can try to isolate its effects and have a better idea of what is causing what. Which I reminded the allergist.
But sometimes it’s hard to effectively advocate for myself, because the trip to the VA hospital is so stressful on my body (3+ hour car ride each way, making sure I have access to bathrooms during the trip, my joints seize up during the ride making it hard to walk, flourescent lights in the hospital, hand sanitizer everywhere [I’m allergic], fragrances everywhere [ditto], stress from dealing with healthcare providers, stress from trying to avoid contact with the antiseptic I’m allergic to, trying to maintain my medication schedule and my eating schedule, etc.). When I have an allergic reaction, it affects my cognitive abilities. Imagine trying to have an intelligent discussion with your doctor during the worst fuzzy-headedness you’ve ever experienced during a cold… I just can’t think straight, and therefore I can’t process what the doctor is telling me and effectively evaluate their plan of action.
In this case, I *should have said* – “Let’s not change anything else while I’m coming off the Xolair. Let’s subtract that and evaluate the reaction for a few months.” But I was not successful in conveying how slowly we needed to proceed.
What happened instead was: I expressed some concerns, the doctor gave me one last Xolair injection, and told me to slowly start stepping down off my other medication (we agreed on one increment/week), and then not to return for my Xolair injection a month later.
So, against my better judgement (never mess with a stable patient), I started decreasing my medication. The first week I had a chronic migraine (for the entire week). So I returned to the full dose the following week. Once the migraine ended and I felt stable again, I reduced my dose by one increment the third week. I’m less clear on what happened after that, because I was slipping into brain fog and lethargy. At some point, I realized two weeks had gone by, because I was refilling my pill caddy again. The next two weeks went by even quicker. The entire month of September came and went, with nothing to show for it on my part.
Cognitive side effects from medications, illnesses, or injuries are insidious because they affect your ability to detect them and your ability to get help.
Crew Dog, onesickvet.com
Initially, I had thought my body was recovering from the trip to the VA, then from the migraine, then from the refinance efforts. But eventually (through the brain fog) I realized that it was probably a result of changing my meds. An additional month went by during which I was not only reducing one medication, but had also discontinued the Xolair, and I had limited cognitive ability and no energy. Like, stand up, accomplish one very small task, and need to sit down/lie down and rest.
Once I figured out what was underlying my symptoms, I contacted my allergist, who agreed to put me back on Xolair while I continue to step-down off the other medication. We’ll see how that goes.
MEANWHILE, in the media, *another* medication I’m on, Zantac (generic name, ranitidine), started getting a lot of attention. At first, it was reported that a few batches of generic Zantac had been found to be contaminated with a substance that is a known cancer-causing substance [NDMA; also see here]. After research into the situation, including reading this FDA statement, I decided to monitor developments but continue to take my prescribed ranitidine. Then Novartis/Sandoz announced that it would do a voluntary recall of its product. Then additional manufacturers announced voluntary recalls [see here for Apotex] and major pharmacies such as Walgreens, Walmart, and Rite Aid announced they would be removing ranitidine from their shelves. I contacted my allergist to determine the manufacturer of my ranitidine, but was unable to get an answer to that specific question. My allergist did, however, talk to the pharmacist at our VA hospital about the situation, and relay information from the pharmacist to me, which I appreciated. Although there has not been an FDA recall of ranitidine, we decided that I would switch to famotidine out of an abundance of caution (and because I have no way of determining the actual manufacturer of the ranitidine I receive from the VA). I am currently waiting for that prescription to be filled.
So, to recap: I tried a new drug. Its effects were subtle but beneficial. Since I had to drive 6-7 hours roundtrip every month to receive the injections, and the doctor did not perceive a dramatic enough improvement, we decided to discontinue the new medication. Overlapping with this change, we also changed another drug. My quality of life took a drastic hit. Now I’m trying to stabilize, but I need to change *a third* medication. Meanwhile, my quality of life has tanked and I’ve spent seven weeks in bed or on the couch.
I’ve lost two months of my life because my new allergist wanted to change my medications and see what happened. I’m tired of being a living medical experiment, although I guess it’s better than being a dead one.
Crew Dog, onesickvet.com
*My impressions of Xolair: It helped me breathe better and gave me (a lot) more energy, but I seemed to be *more* reactive to foods and smells. We had hoped I would be *less* reactive to foods and smells.